IVF (FERTILITY)
Fertility Details For Trans Women
Transition & Fertility
A gender affirming transition — including the hormones and the surgeries considered — can have lasting impacts on one’s fertility. If possible it’s best to think through these downstream impacts to fertility before the transition process begins.
Estrogen & Hormone Therapy
As part of transition, trans women typically take estrogen and sometimes androgen blockers.
Estrogen in particular has harmful effects on sperm production. In many cases those effects can cause permanent damage, impeding the ability to produce sperm.
In some cases, though, people are able to produce sperm after coming off of estrogen. When asked to come off estrogen for between three to six months, it is occasionally possible to produce some sperm, but when interviewing doctors about their clinical experience, they say that it’s usually only a very small amount of sperm that can be produced, meaning that conception without medical assistance isn’t likely — IUI or, most likely, IVF will be required.
But there is very little data about the amount of time one should be off of estrogen before trying to collect sperm, or what the rates of sperm production are after varying periods of exposure to estrogen. A typical spermatogenesis or sperm growth cycle is at least three months, so there’s no reason to expect results before then.
Gender Affirming Surgery & Fertility
Gender affirming surgery, depending on which surgery is chosen, can have permanent impacts on a persons’ fertility. Namely “bottom surgery,” or removing a persons testes, will permanently compromise that person’s fertility unless fertility preservation is undertaken beforehand.
Reproductive Options
Transfeminine individuals have several reproductive options depending on their stage of transition, their social situation, and whether or not they have undergone some form of fertility preservation. The main options are unassisted conception with a partner, IUI with a partner who has a uterus, and IVF either with a partner who has a uterus or a gestational carrier. In the future, uterine transplant might be a possible way that a transfeminine woman could carry a pregnancy.
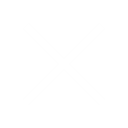
Below we characterize the rates of success, the costs and the burden for each treatment. Typically, the cost, burden and rates of success tend to increase with each new approach. That said we should point out that the “success rates” below are built from datasets that comprise infertile, cisgender, heterosexual couples. Its plausible that rates of success could look dramatically different (better or worse) for trans women.
Unassisted Conception
Although in most cases estrogen impacts one’s ability to produce sperm, it is sometimes possible for a trans feminine individual to come off of estrogen for a period of months and, if they are willing and able to engage in penetrative intercourse with a partner, conceive a pregnancy without medical assistance.
Of course, if someone has not yet started hormonal transition and also has not had their testes removed, then unassisted conception is possible as well.
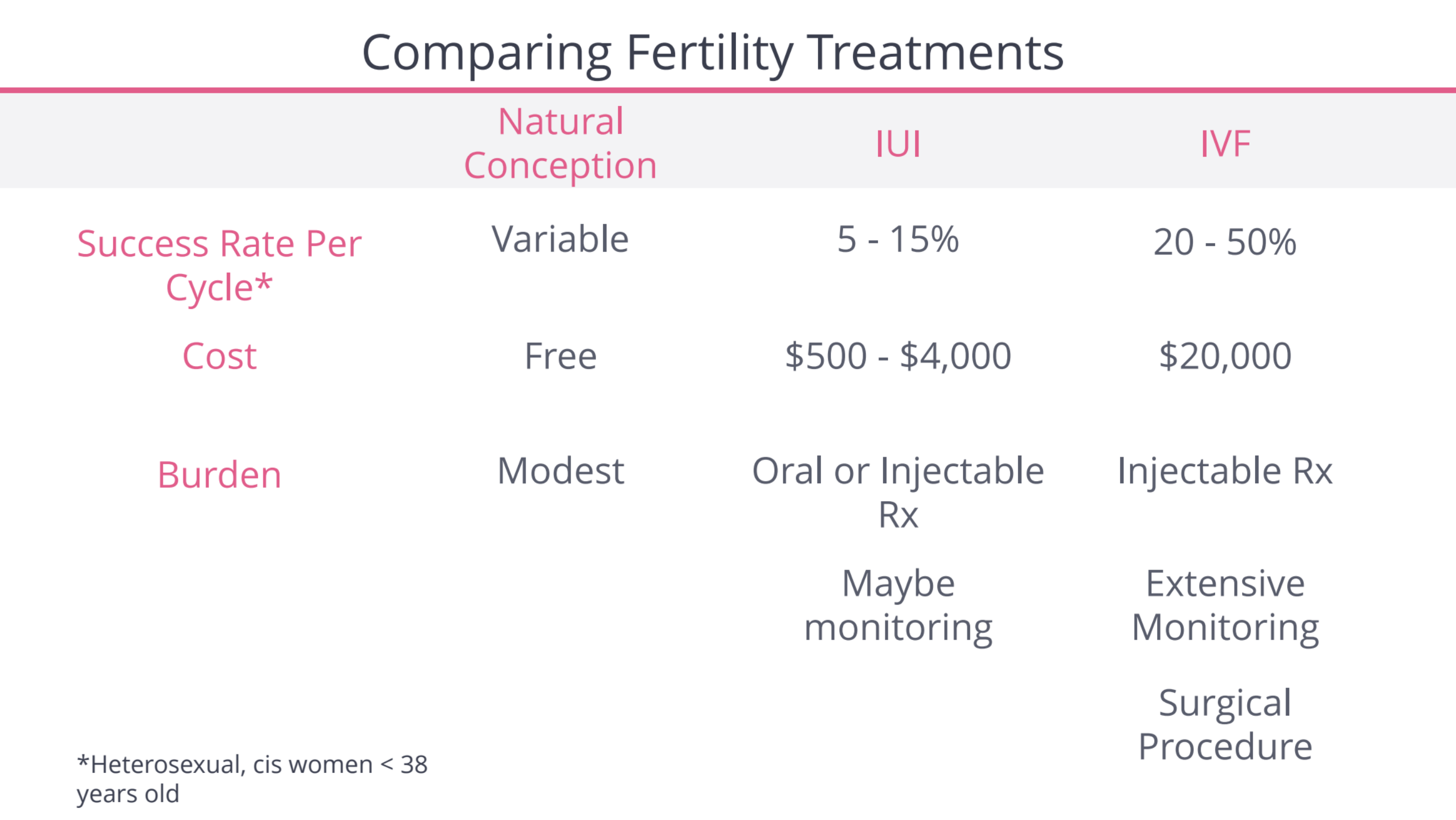
While it’s far from a perfect reference point, the data below collected from cisgender, heterosexual couples shows that if unassisted conception hasn’t happened in the first six to twelve months, the odds of it happening in any subsequent months are fairly low.
For cisgender, heterosexual couples, the definition of medical infertility kicks in after 6 months of trying to conceive after age 35, or a year of trying until age 35. Trans women who have been on hormones should seek guidance from a fertility specialist before this time frame, though, to ensure that sperm counts are acceptable for trying naturally.
IUI or Artificial Insemination
IUI, which is also called intrauterine insemination or artificial insemination, is another avenue for trans feminine individuals who have a partner with a uterus.
This is a somewhat simple procedure where sperm in injected directly into the uterus of a partner who would carry the pregnancy.
The sperm used in IUI would ideally be sperm preserved or banked prior to hormonal transition, but it’s also possible for some individuals to do IUI with sperm they produce after coming off of estrogen.
IUI success rates vary and depend most closely on the age of the person who will be carrying a pregnancy, as you can see below. Unfortunately this data is from cisgender women with a history of infertility.
Fertility Details For Trans Women
Transition & Fertility
A gender affirming transition — including the hormones and the surgeries considered — can have lasting impacts on one’s fertility. If possible it’s best to think through these downstream impacts to fertility before the transition process begins.
Estrogen & Hormone Therapy
As part of transition, trans women typically take estrogen and sometimes androgen blockers.
Estrogen in particular has harmful effects on sperm production. In many cases those effects can cause permanent damage, impeding the ability to produce sperm.
In some cases, though, people are able to produce sperm after coming off of estrogen. When asked to come off estrogen for between three to six months, it is occasionally possible to produce some sperm, but when interviewing doctors about their clinical experience, they say that it’s usually only a very small amount of sperm that can be produced, meaning that conception without medical assistance isn’t likely — IUI or, most likely, IVF will be required.
But there is very little data about the amount of time one should be off of estrogen before trying to collect sperm, or what the rates of sperm production are after varying periods of exposure to estrogen. A typical spermatogenesis or sperm growth cycle is at least three months, so there’s no reason to expect results before then.
Gender Affirming Surgery & Fertility
Gender affirming surgery, depending on which surgery is chosen, can have permanent impacts on a persons’ fertility. Namely “bottom surgery,” or removing a persons testes, will permanently compromise that person’s fertility unless fertility preservation is undertaken beforehand.
Reproductive Options
Transfeminine individuals have several reproductive options depending on their stage of transition, their social situation, and whether or not they have undergone some form of fertility preservation. The main options are unassisted conception with a partner, IUI with a partner who has a uterus, and IVF either with a partner who has a uterus or a gestational carrier. In the future, uterine transplant might be a possible way that a transfeminine woman could carry a pregnancy.
Below we characterize the rates of success, the costs and the burden for each treatment. Typically, the cost, burden and rates of success tend to increase with each new approach. That said we should point out that the “success rates” below are built from datasets that comprise infertile, cisgender, heterosexual couples. Its plausible that rates of success could look dramatically different (better or worse) for trans women.
Unassisted Conception
Although in most cases estrogen impacts one’s ability to produce sperm, it is sometimes possible for a trans feminine individual to come off of estrogen for a period of months and, if they are willing and able to engage in penetrative intercourse with a partner, conceive a pregnancy without medical assistance.
Of course, if someone has not yet started hormonal transition and also has not had their testes removed, then unassisted conception is possible as well.
While it’s far from a perfect reference point, the data below collected from cisgender, heterosexual couples shows that if unassisted conception hasn’t happened in the first six to twelve months, the odds of it happening in any subsequent months are fairly low.
For cisgender, heterosexual couples, the definition of medical infertility kicks in after 6 months of trying to conceive after age 35, or a year of trying until age 35. Trans women who have been on hormones should seek guidance from a fertility specialist before this time frame, though, to ensure that sperm counts are acceptable for trying naturally.
IUI or Artificial Insemination
IUI, which is also called intrauterine insemination or artificial insemination, is another avenue for trans feminine individuals who have a partner with a uterus.
This is a somewhat simple procedure where sperm in injected directly into the uterus of a partner who would carry the pregnancy.
The sperm used in IUI would ideally be sperm preserved or banked prior to hormonal transition, but it’s also possible for some individuals to do IUI with sperm they produce after coming off of estrogen.
IUI success rates vary and depend most closely on the age of the person who will be carrying a pregnancy, as you can see below. Unfortunately this data is from cisgender women with a history of infertility.
Additionally, IUI success rates and costs vary dramatically depending upon which, if any, fertility medication the person carrying a pregnancy has taken. Similarly, the rate of risk for a “multiple pregnancy” varies depending upon which drug is used. The table below illustrates the point, though the success rate data it contains comes from infertile, cisgender, heterosexual couples. It’s plausible that rates may be different for couples where one partner is a trans woman.
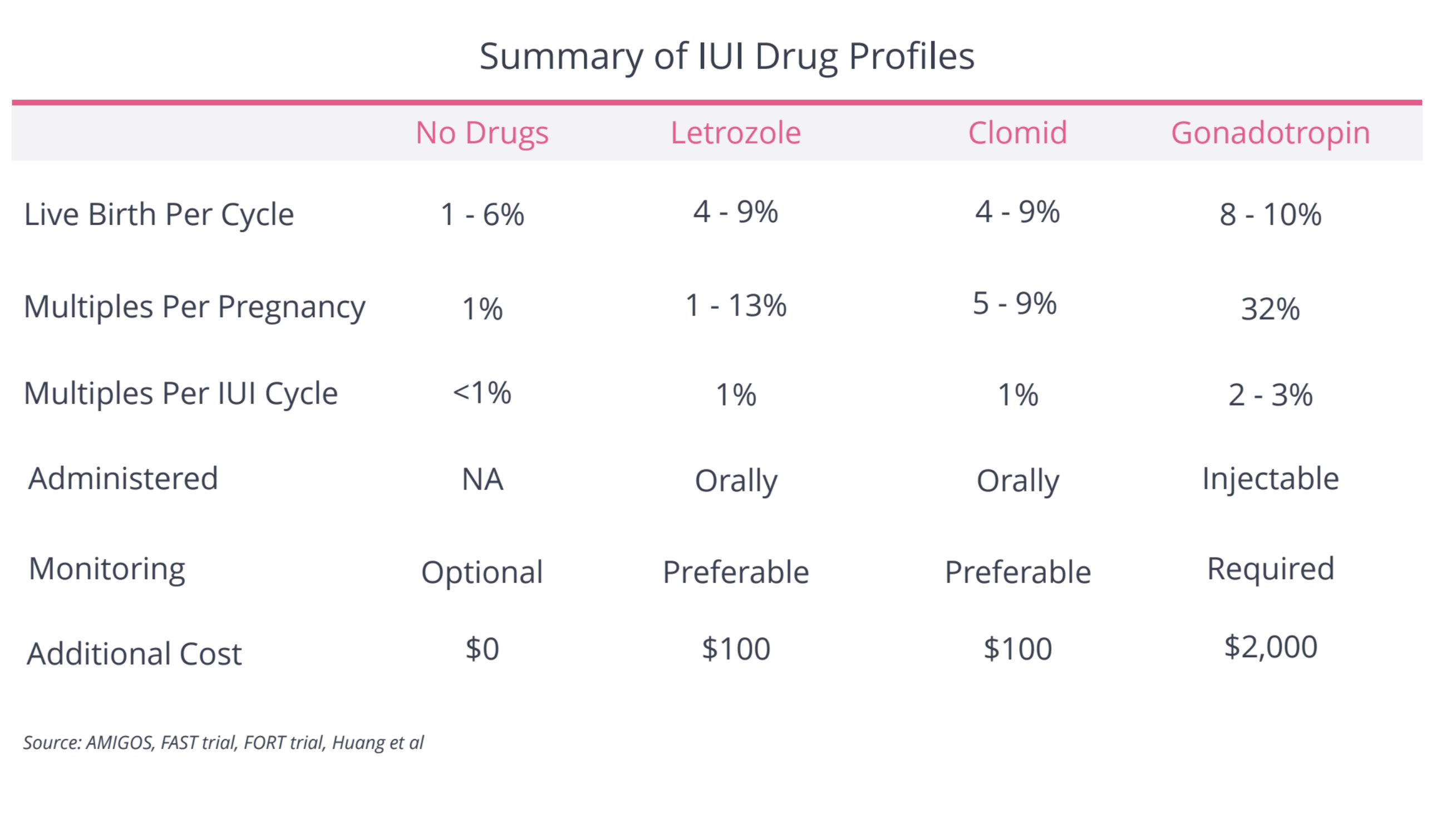
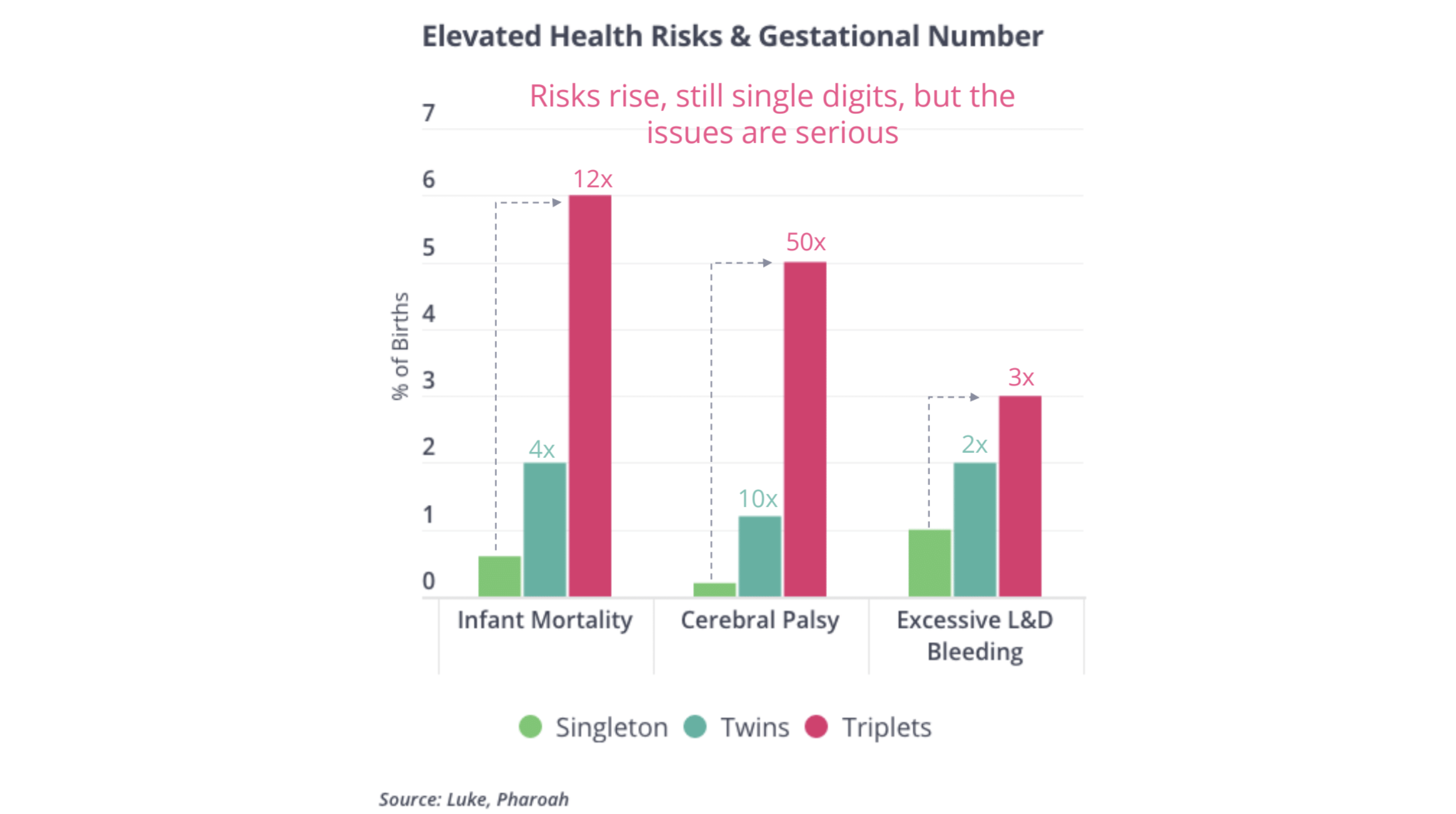
It’s worth noting that we characterize carrying a multiple gestation pregnancy as a “risk” because it tends to increase the odds there will be a major complications with the pregnancy and delivery.
If sperm was banked before transition, and that sperm appeared to be of high quality (see our section on the semen analysis below), then IUI success rates might be more analogous to success rates in cis lesbians, who are presumed not have an underlying fertility problem.
Data shows that cis lesbians enjoy higher success rates than their counterparts who were studied in infertile, heterosexual couples. Success rates from cis lesbians can be seen below. By the 5th IUI, more than half became pregnant, which is a staggeringly high rate of success for IUI.
If sperm has not been banked prior to transition, the ability to engage in IUI will depend on the quality of sperm that is produced after going off of estrogen. Based on doctors’ clinical experience, not data, they say that there is rarely enough sperm produced after coming off of estrogen to consider an IUI cycle.
As you can see in the data below (which was focused on cisgender men), rates of IUI success go down once sperm counts have crossed below certain thresholds. Below you can see how IUI success rates coincide with a lower total motile count, or TMC, which is the number of sperm that swim forward.
IVF
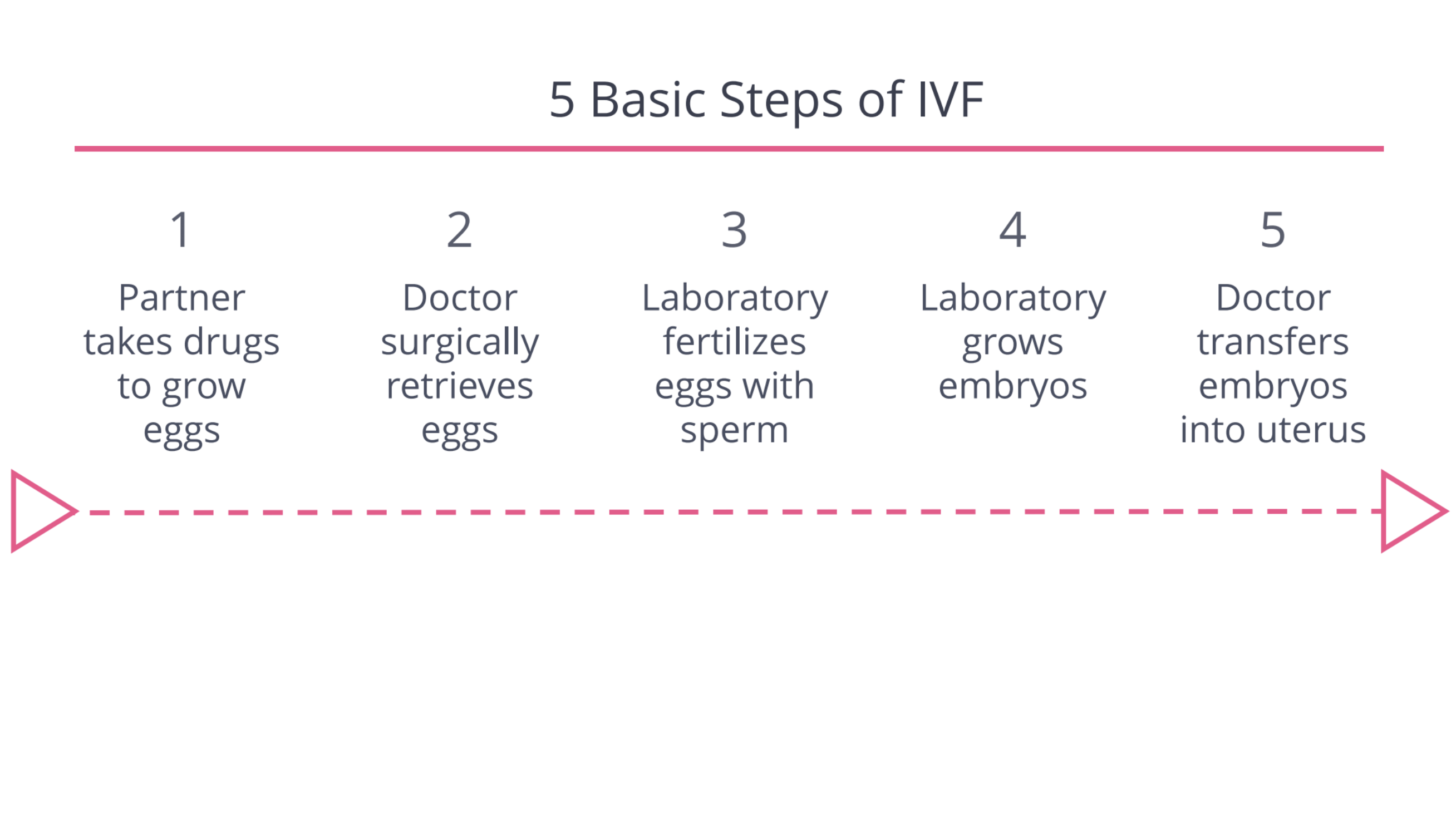
IVF, or in vitro fertilization, entails fertilizing eggs with sperm in a petri dish before placing a resulting embryo into the uterus of a person who will carry the pregnancy. This requires that one person use fertility hormones to prompt the ovaries to produce a large number of eggs and eventually have a surgical procedure to remove those eggs.
Generally speaking, the two crucial points to note are that IVF is expensive and seldom works the first time. As for cost, as you can see below, in most major US cities, each IVF cycle costs around $20,000. Below you’ll find our section on how to think through paying for care.
Unfortunately, the first IVF cycle often does not work. As you can see from the data below, success rates are often tied to the age of the person whose eggs are being used.

A fundamental question is how many IVF cycles a person will need to undergo to have a baby. As you can see from the data below (captured from mostly cisgender infertile people), cycles #2 – 5 can be either worthwhile, or somewhat less-productive, depending upon the age of the partner whose eggs are being used.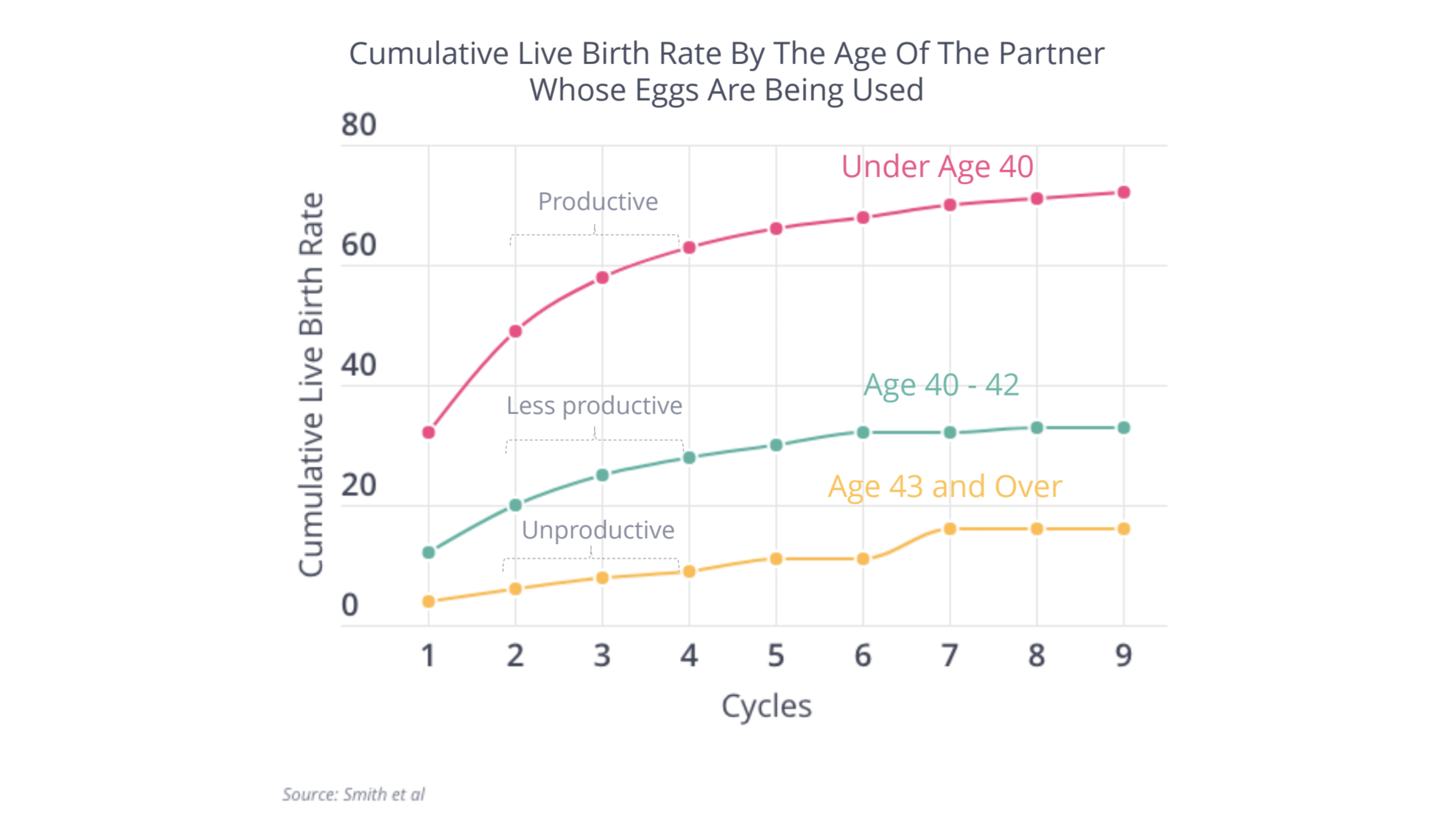
Sperm for IVF
The sperm that is used for IVF can come from frozen sperm preserved before transition, from sperm produced after discontinuing hormones like estrogen, or from a sperm donor.
In the case that ejaculation is not possible, or no sperm is found in semen that is ejaculated, it is sometimes possible to surgically retrieve sperm directly from the testes using techniques like testicular sperm extraction or TESE. When these procedures work, a very small number of sperm are typically extracted, meaning that the only way to effectively use this sperm is through IVF and a special fertilization technique called ICSI, whereby a single sperm is injected directly into a single egg.
As you can see in the data below (based upon cisgender men), IVF success rates tend to be lower when this surgical approach is requred.
Third Party IVF
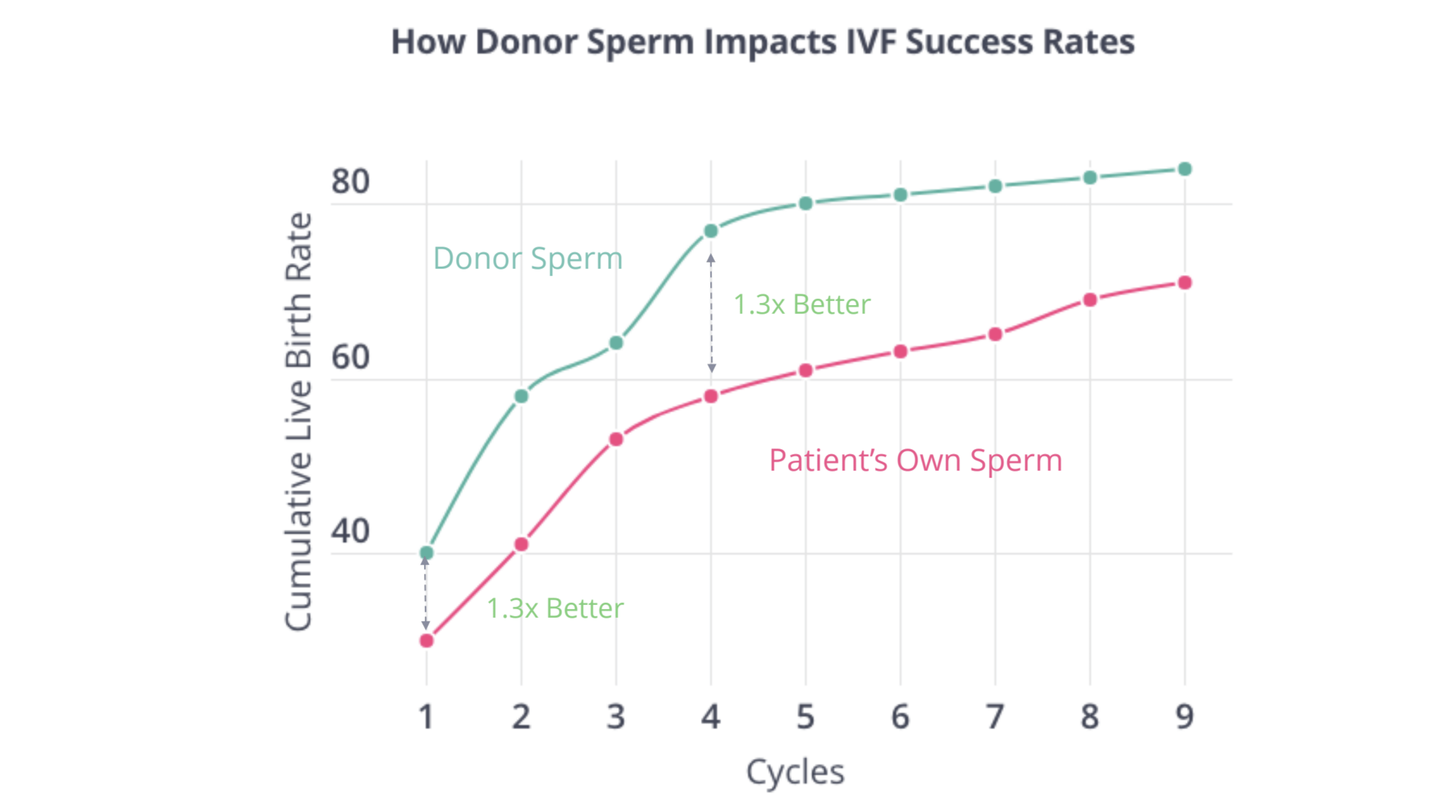
It’s possible to do IVF with a partner who has eggs and a uterus, but it’s also possible to use donor eggs, donor sperm, the uterus of a gestational carrier, or any combination of those components.
When there’s an issue with sperm and donor sperm is used instead, IVF success rates often improve.
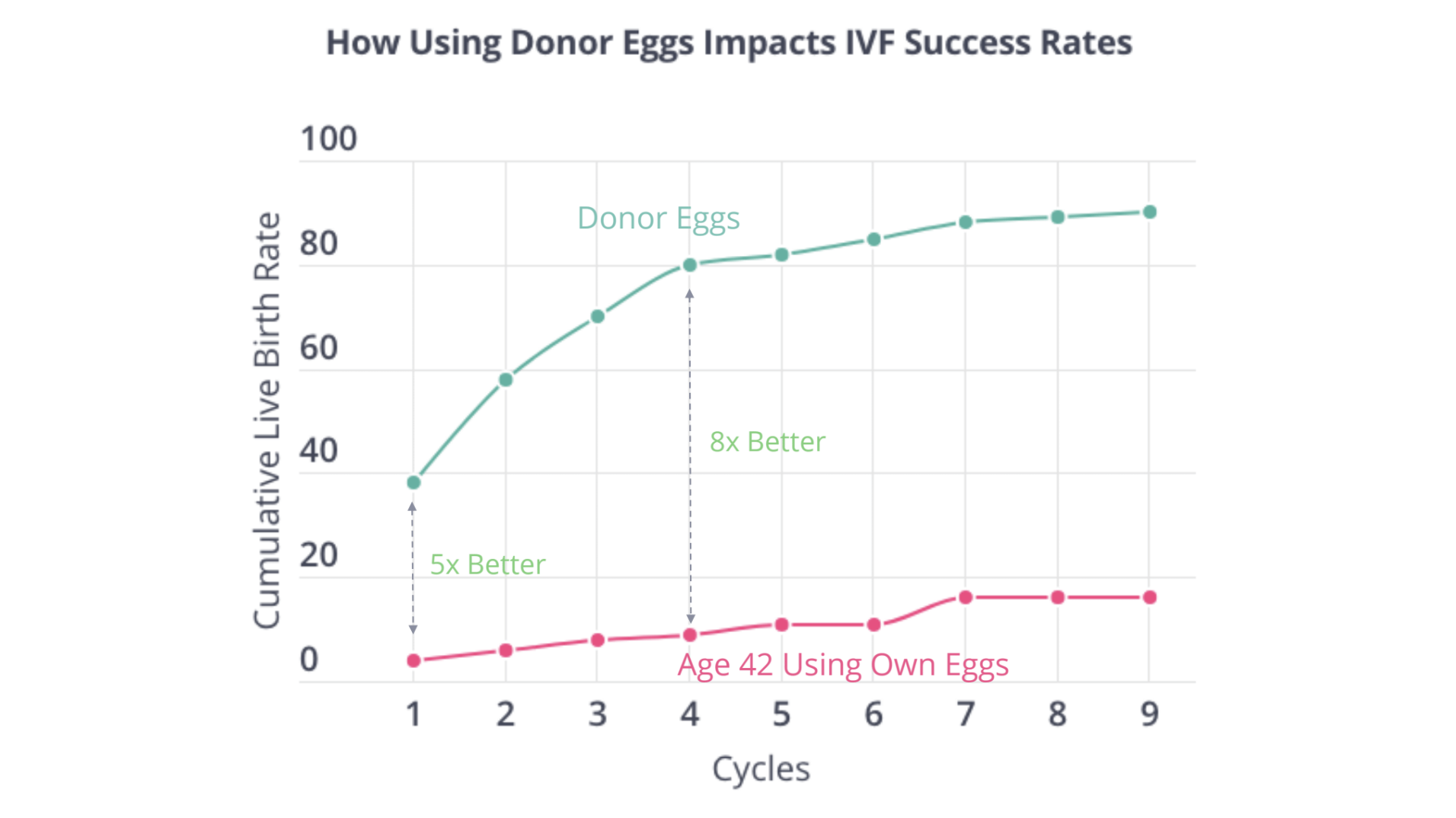
In the case of an egg-related issue, the gains made by using donor eggs can be even more remarkable — they can increase IVF success rates by five to eight times in some cases. The data below is from cisgender women at 42-years-old.